
I did my 3 month A1c which coincides with 11 weeks of taking Januvia.
It came out to be 5.6%. This is .1% higher than what I achieved with bolus insulin 3 or 4 times a day, so while it wasn't as low as I was hoping it would be, given my meter results, it confirmed that Januvia was giving me PP control very similar to what I was getting with insulin.
I also had some blood tests taken to see if Januvia was affecting my immune system in any way that was visible on simple tests. I'll be discussing that with the Endo this coming week.
From the little I know about interpreting blood tests, it looks to me like my white blood cell count is a bit higher than it was in the summer when I last had the measured, back when the doctor thought my joint inflammation might be from an infection. I'm not sure what that means.
I'm also not sure if the changes in the immune system which are made by suppressing DPP-4 would be visible on the CBC/Diff lab test. It might need a much more specialized test which isn't available to us humble guinea pigs taking these brand new, near-experimental drugs.
I have been having killer sinus headaches with increasing frequency over the past months, and I recently realized that these, too, are a known side effect of Januvia. That, combined with how painful my fingertips have become with only a limited amount of testing (1-3 tests a day) which has made me worry about healing problems, is motivating me to stop the Januvia and see what happens to my bgs.
I'd thought of asking the endo about trying Byetta, but the Diabetes Monitor Byetta Information Page informs me that sinus headaches are a common side effect of Byetta, too, as is feeling like crap, and enhanced allergies, both things I can do without. So I'm not so sure I want to try it after all.
It sucks that they can't deliver GLP-1 in pill form straight to the digestive tract where it belongs rather than having to inject it into the fat layer where it upsets the immune system.
March 31, 2007
March 25, 2007
Does Januvia Slow Wound Healing? Does it Cause Cancer?
UPDATE (April 2, 2013): Before you take Byetta, Victoza, Onglyza, or Januvia please read about the new research that shows that they, and probably all incretin drugs, cause severely abnormal cell growth in the pancreas and precancerous tumors. You'll find that information HERE.
Note to visitors in 2009:
This is a very old blog post. For the most recent information about Januvia's impact on cancers of the lung, prostate, ovary and melanoma, please visit this page:
Januvia
where you will find many links to journal research about the impact of DPP-4 and cancer in the section headed "Research Connecting DPP-4 and Cancer."
Below is the original post which was made on 3/25/2007:
====================================================
Now that I've taken Januvia for a few months and had a chance to do some more research on it, a couple of issues have come up that are making me rethink whether it is wise to take it, even though I am getting such good results.
My experience with Slow Wound Healing
After I'd been taking Januvia for a few weeks I cut myself (not very seriously) while cooking. But it seemed to take forever for the wound to heal. At the same time I noticed that I was getting sore spots on my fingers where I was testing my blood sugar. This really was unusual. I'd been testing 6-8 times a day while on insulin and my fingers never hurt. Suddenly they were getting red and sore.
This raised the concern for me that the slight alterations to the immune system, and possibly other effects of DDP-4 were affecting healing. I posted about this on the Januvia blog at http://diabetes.blog.com and someone chimed in that they had also noticed slow wound healing which went away when they stopped the Januvia.
This could be a VERY serious concern, especially if you were to have surgery while taking this drug. I asked a surgeon about this when I was considering some elective surgery, and she told me that I'd have to ask my endocrinologist because she prescribed the drug. However, my endo knows only what is in the prescribing information, which doesn't mention any effect on the immune system except that Januvia makes some minor changes in white blood cell levels the importance of which is unknown. (How's that for avoiding the issue. Why isn't it known?)
The relevant data about how DPP-4 inhibition affects the immune system is hidden in scholarly studies of the effects of inhibiting DPP-4 which make it clear that DPP-4 inhibition does weaken immune response. I think, though my understanding of molecular biology isn't strong enough to be sure, that DPP-4 inhibition may have some effect on the process of healing itself.
If you've experienced any wound healing problems with Januvia, please contact me. Click on my profile and use the email address there, rather than posting a comment, if you want a reply.
I have seen it argued that since Januvia turns down the immune system, it might be extremely useful for people with diabetes who have inflammatory conditions like artery disease, gum disease, arthritis, and of course, inflammation of the beta cells. This may be true. Since inflammation is supposed to be what leads to heart attacks, downregulation of inflammation in the arteries could be good. It's also true that inflammation in the beta cells may be part of what kills them in Type 2 diabetes. There are also some initial studies showing that DPP-4 inhibition helps with autoimmune rheumatoid arthritis. However, for those of us who do not have inflammatory conditions--as revealed by tests like CRP (C-Reactive Protein), SED rate, etc.-- turning down the immune system might allow the random cancer cells we all produce from time to time to avoid detection and destruction.
Since I'm a melanoma survivor, I'm NOT happy about electively suppressing the same enzyme DPP-4 that melanoma cells suppress.
In an ideal world, we could trust the drug companies to test these drugs in ways that would assure us we weren't going to wake up in ten years and find out that this wonder drug increased our chances of getting cancer ten times. But this is a pill that retails for $5 a pill, sold by a drug company that really needs some new blockbuster drugs to keep its billion dollar profits going. They hit the market first with their oral incretin hormone pill which gives them a huge sales advantage. How likely are they to study the possibility that their fancy new drug has a fatal side effect that takes ten years to develop? The longest test of Januvia lasted just shy of two years.
I'm thinking I might talk to my doctor about switching to Byetta now that I know that incretin drugs are very effective for me. Byetta does not suppress enzymes and shouldn't have any direct effect on the immune system. (But then there is the concern about creating antibodies since it's injected. There's always something . . .)
NEW INFORMATION ABOUT JANUVIA AND CANCER
added September/2008:
http://diabetesupdate.blogspot.com/2008/09/more-evidence-connects-januvia-to.html
Note to visitors in 2009:
This is a very old blog post. For the most recent information about Januvia's impact on cancers of the lung, prostate, ovary and melanoma, please visit this page:
Januvia
where you will find many links to journal research about the impact of DPP-4 and cancer in the section headed "Research Connecting DPP-4 and Cancer."
Below is the original post which was made on 3/25/2007:
====================================================
Now that I've taken Januvia for a few months and had a chance to do some more research on it, a couple of issues have come up that are making me rethink whether it is wise to take it, even though I am getting such good results.
My experience with Slow Wound Healing
After I'd been taking Januvia for a few weeks I cut myself (not very seriously) while cooking. But it seemed to take forever for the wound to heal. At the same time I noticed that I was getting sore spots on my fingers where I was testing my blood sugar. This really was unusual. I'd been testing 6-8 times a day while on insulin and my fingers never hurt. Suddenly they were getting red and sore.
This raised the concern for me that the slight alterations to the immune system, and possibly other effects of DDP-4 were affecting healing. I posted about this on the Januvia blog at http://diabetes.blog.com and someone chimed in that they had also noticed slow wound healing which went away when they stopped the Januvia.
This could be a VERY serious concern, especially if you were to have surgery while taking this drug. I asked a surgeon about this when I was considering some elective surgery, and she told me that I'd have to ask my endocrinologist because she prescribed the drug. However, my endo knows only what is in the prescribing information, which doesn't mention any effect on the immune system except that Januvia makes some minor changes in white blood cell levels the importance of which is unknown. (How's that for avoiding the issue. Why isn't it known?)
The relevant data about how DPP-4 inhibition affects the immune system is hidden in scholarly studies of the effects of inhibiting DPP-4 which make it clear that DPP-4 inhibition does weaken immune response. I think, though my understanding of molecular biology isn't strong enough to be sure, that DPP-4 inhibition may have some effect on the process of healing itself.
If you've experienced any wound healing problems with Januvia, please contact me. Click on my profile and use the email address there, rather than posting a comment, if you want a reply.
Could Januvia Promote Cancer?
Because suppressing DPP-4 weakens the immune system, I have another very serious concern about whether it might promote cancer. DPP4 is also suppressed by melanoma cells and prostate cancer cells, and it is speculated that this might be what allows these tumors to fend off the immune system cells that are supposed to kill them. Rats fed a very high dose of Januvia (60 times the normal amount) did develop liver cancer, though mice did not. This is not trivial and only a lot of time will reveal the impact of DPP4 suppression on people.I have seen it argued that since Januvia turns down the immune system, it might be extremely useful for people with diabetes who have inflammatory conditions like artery disease, gum disease, arthritis, and of course, inflammation of the beta cells. This may be true. Since inflammation is supposed to be what leads to heart attacks, downregulation of inflammation in the arteries could be good. It's also true that inflammation in the beta cells may be part of what kills them in Type 2 diabetes. There are also some initial studies showing that DPP-4 inhibition helps with autoimmune rheumatoid arthritis. However, for those of us who do not have inflammatory conditions--as revealed by tests like CRP (C-Reactive Protein), SED rate, etc.-- turning down the immune system might allow the random cancer cells we all produce from time to time to avoid detection and destruction.
Since I'm a melanoma survivor, I'm NOT happy about electively suppressing the same enzyme DPP-4 that melanoma cells suppress.
In an ideal world, we could trust the drug companies to test these drugs in ways that would assure us we weren't going to wake up in ten years and find out that this wonder drug increased our chances of getting cancer ten times. But this is a pill that retails for $5 a pill, sold by a drug company that really needs some new blockbuster drugs to keep its billion dollar profits going. They hit the market first with their oral incretin hormone pill which gives them a huge sales advantage. How likely are they to study the possibility that their fancy new drug has a fatal side effect that takes ten years to develop? The longest test of Januvia lasted just shy of two years.
I'm thinking I might talk to my doctor about switching to Byetta now that I know that incretin drugs are very effective for me. Byetta does not suppress enzymes and shouldn't have any direct effect on the immune system. (But then there is the concern about creating antibodies since it's injected. There's always something . . .)
NEW INFORMATION ABOUT JANUVIA AND CANCER
added September/2008:
http://diabetesupdate.blogspot.com/2008/09/more-evidence-connects-januvia-to.html
March 23, 2007
This is What Diabetes Sounds Like!
Too much blood sugar might be what makes this new album so sweet, but whatever the explanation, I'm hooked. It has been years since I've bought an album I enjoyed this much. Elliot Yamin (who finished third on American Idol last year) has a beautiful voice, and even more importantly, he has impeccable taste. These songs stick in your head all day.
Elliot has Type 1 diabetes and wears a pump. He's used his new-found celebrity to promote the JDRF and has spent considerable time with young people with diabetes serving as a role model.
What I love the most about this album is that it is optimistic, idealistic, full of love songs without an ironic twist. It's been years since anyone has dared to be this open and loving in public. I hope he becomes a huge star. It's time the media featured someone besides angsty spoiled brats.
You can listen to some of Elliott's new album here:
http://www.myspace.com/elliottyamin
Here's the video:
http://youtube.com/watch?v=SEOaAIF5hsA
It's independently produced so buying it supports the artist. If you enjoy it and want to do something back for Elliott consider making a contribution to The Juvenile Diabetes Research Foundation. I did.
http://www.jdrf.org/
Elliot has Type 1 diabetes and wears a pump. He's used his new-found celebrity to promote the JDRF and has spent considerable time with young people with diabetes serving as a role model.
What I love the most about this album is that it is optimistic, idealistic, full of love songs without an ironic twist. It's been years since anyone has dared to be this open and loving in public. I hope he becomes a huge star. It's time the media featured someone besides angsty spoiled brats.
You can listen to some of Elliott's new album here:
http://www.myspace.com/elliottyamin
Here's the video:
http://youtube.com/watch?v=SEOaAIF5hsA
It's independently produced so buying it supports the artist. If you enjoy it and want to do something back for Elliott consider making a contribution to The Juvenile Diabetes Research Foundation. I did.
http://www.jdrf.org/
March 21, 2007
Exubera Update
If you'll remember, back when Pfizer launched Exubera, the inhaled insulin, with a lot of press hype, I was interviewed by Business Week as a "typical patient" and I quoted (very vaguely) about why I thought Exubera was a bad idea for people with diabetes.
It looks like I was onto something.
Today the AP is carrying a story about how endocrinologists have proved resistant to Pfizer's push to market this expensive, potentially dangerous form of insulin.
Here's a quote from the article:
" ''I think Pfizer will wish they had never gotten into this. I doubt they'll regain their investment,'' said Dr. John Buse, president-elect of the American Diabetes Association, who participated in Exubera's trials. ''There is no advantage to Exubera and there may be a safety risk. I see it as my job to talk people out of (using) it.'' "
Pfizer's main concern is profits, so they're responding to the refusal of the endocrinologists to prescribe the drug by hiring hundreds of supposed "diabetes educators" to market the drug to general practitioners--doctors with little if any expertise in prescribing insulin, who can, presumably, be more easily talked into putting their patients on the drug.
What's wrong with Exubera you may ask?
1. A good possibility that it causes long-term lung damage. You only have one set of lungs and if you screw them up, life is unpleasant and short.
2. This is a meal time (bolus) insulin but it is dosed by the patient's body weight. So the dosage does not correlate to the grams of carbs in the meal. This makes it impossible for people using it to achieve normal blood sugars.
In contrast, Novolog can be matched very closely to the number of grams of carbohydrate in a meal, as can regular (R) insulin. This makes it possible to achieve completely normal blood sugars using them, especially if you keep carbohydrate amounts low to moderate.
3. Expense. This insulin cost far more than the other insulins on the market.
There are some versions of oral insulin in the testing pipeline that don't need to be inhaled. They may prove to be a better choice for people who are needle-phobic. Unfortunately, the dosing issue may still be a problem with those products. And the very high cost may be an even bigger problem.
It looks like I was onto something.
Today the AP is carrying a story about how endocrinologists have proved resistant to Pfizer's push to market this expensive, potentially dangerous form of insulin.
Here's a quote from the article:
" ''I think Pfizer will wish they had never gotten into this. I doubt they'll regain their investment,'' said Dr. John Buse, president-elect of the American Diabetes Association, who participated in Exubera's trials. ''There is no advantage to Exubera and there may be a safety risk. I see it as my job to talk people out of (using) it.'' "
Pfizer's main concern is profits, so they're responding to the refusal of the endocrinologists to prescribe the drug by hiring hundreds of supposed "diabetes educators" to market the drug to general practitioners--doctors with little if any expertise in prescribing insulin, who can, presumably, be more easily talked into putting their patients on the drug.
What's wrong with Exubera you may ask?
1. A good possibility that it causes long-term lung damage. You only have one set of lungs and if you screw them up, life is unpleasant and short.
2. This is a meal time (bolus) insulin but it is dosed by the patient's body weight. So the dosage does not correlate to the grams of carbs in the meal. This makes it impossible for people using it to achieve normal blood sugars.
In contrast, Novolog can be matched very closely to the number of grams of carbohydrate in a meal, as can regular (R) insulin. This makes it possible to achieve completely normal blood sugars using them, especially if you keep carbohydrate amounts low to moderate.
3. Expense. This insulin cost far more than the other insulins on the market.
There are some versions of oral insulin in the testing pipeline that don't need to be inhaled. They may prove to be a better choice for people who are needle-phobic. Unfortunately, the dosing issue may still be a problem with those products. And the very high cost may be an even bigger problem.
March 18, 2007
Dieting on Januvia
UPDATE (April 2, 2013): Before you take Byetta, Victoza, Onglyza, or Januvia please read about the new research that shows that they, and probably all incretin drugs, cause severely abnormal cell growth in the pancreas and precancerous tumors. You'll find that information HERE.
Original Post:
I have maintained my 30 lb weight loss for 4 years by following one simple rule. When my weight goes 3 lbs over target, I diet back to goal. It only takes a couple of weeks to lose 3 lbs. Losing more than that swiftly becomes almost overwhelming.
The only way I can lose weight now is by restricting calories. At my age, 58, and at my size, small, the body only needs 1600 calories to maintain, so to lose weight I have to eat almost nothing. So I kicked off the diet 2 weeks ago with two days at 1000 calories. I was very hungry during those days, which is to be expected at the beginning of any diet, but by day 3, I'd stopped being hungry and I've done extremely well since then.
I log everything I eat in LifeForm software and use a food scale to check portion sizes. This is anal to the nth degree, but it works. Through this 2 week period, my daily input has averaged 1145 calories, broken out into 95 grams of carbs and 11 grams of fiber, for a net carb intake of 84 grams. Protein grams average 57, and fat grams 61.
The 1145 calories is significantly less than what I had intended to eat, which brings me to my point. Januvia , because it has an impact on stomach emptying, does seem to make it a bit easier to lose weight--if you are willing to restrict food. Unlike metformin, it does not cause weight loss without trying when you first start it. In fact, as I've documented, I gained a few pounds after taking it for 2 months. But because delayed stomach emptying makes me feel full when I've eaten relatively small amounts of food, it seems to make it much easier to eat at a low calorie level I have found impossible in the past.
In the past, when I've dieted, I've always cut my carbs way down. But what I found during the first few days on this diet, when I was restricting carbs more stringently, was this: if I don't eat enough carbs to go over the threshold that stimulates GLP-1-mediated first phase insulin response, my blood sugars throughout the day will be higher than if I do eat those carbs. So I do a lot better as far as blood sugars go, while taking Januvia, when eating 30 grams per meal than I do eating 10.
I also find that, as I've learned in the past, my fasting bgs are a bit better if I eat a slightly carby snack before bed--say a pretzel log. But since I've also learned that I diet best if I only eat at meals, I haven't been eating in the evening, so my fasting bg is in the 90s again, rather than the 80s. However, during the day, my blood sugar two hours after eating and until I eat again remains in the low 80s, sometimes even the 70s.
As a result, my total meter average has declined to 94 over the past 2 weeks, from 96 for the month, but my fasting bg for the week is up to 90 from 88 while after meals average is down 1 to 99 from 100. Since my meter average at the end of the period when I was taking insulin was 103, I'm very happy with all these figures (I didn't have a meter that distinguished before and after meals back then.)
After 2 weeks, I am back o my target weight, which suggests that some of the weight gain was water weight, but I'm doing so well with the diet, I'm going to put in another week and see how much lower I can get since it's not all that difficult. However, before I do that, I'm going to eat normally today and possibly tomorrow.
That's because eating at such a low calorie level is likely to slow my metabolism, a common problem with diets, and I don't want to start gaining weight when I go back to eating the 1600 calorie a day diet on which I've maintained so nicely through the last 4 years.
My final comment is that going from 12 grams of carbs (on a LC regimen) to a 30 gram carb intake makes the difference between a diet that feels very stringent and one where I literally, as they say in the crappy infomercials, "lose weight eating all my favorite foods." I've been eating toast for breakfast and 100 g of diet ice cream for dessert, with other occasional "treats" including 4 ounces of a bakery eclair. All weighed and counted--and with no blood sugar over 105 at 1 hour except once, when I saw 119 mg/dl.
That 119 mg/dl occurred several hours after eating, when I got very dizzy from too low a blood pressure and ended up with a counterregulatory response that pushed up both blood pressure, pulse, and blood sugar. Not after eating carbs! It looks like my weird surge of high blood pressure is fading some and starting to see the medication pushing me too low which is what has happened in the past.
Meanwhile, the seedlings are growing by the window sill, the 15 inches of snow on my back yard are enjoying one last wintry blast before next week's temperatures rise into he 40s and 50s, and pretty soon I'll be out in my garden, using up a lot more physical energy and reveling in the wonder that is the New England spring!
Original Post:
I have maintained my 30 lb weight loss for 4 years by following one simple rule. When my weight goes 3 lbs over target, I diet back to goal. It only takes a couple of weeks to lose 3 lbs. Losing more than that swiftly becomes almost overwhelming.
The only way I can lose weight now is by restricting calories. At my age, 58, and at my size, small, the body only needs 1600 calories to maintain, so to lose weight I have to eat almost nothing. So I kicked off the diet 2 weeks ago with two days at 1000 calories. I was very hungry during those days, which is to be expected at the beginning of any diet, but by day 3, I'd stopped being hungry and I've done extremely well since then.
I log everything I eat in LifeForm software and use a food scale to check portion sizes. This is anal to the nth degree, but it works. Through this 2 week period, my daily input has averaged 1145 calories, broken out into 95 grams of carbs and 11 grams of fiber, for a net carb intake of 84 grams. Protein grams average 57, and fat grams 61.
The 1145 calories is significantly less than what I had intended to eat, which brings me to my point. Januvia , because it has an impact on stomach emptying, does seem to make it a bit easier to lose weight--if you are willing to restrict food. Unlike metformin, it does not cause weight loss without trying when you first start it. In fact, as I've documented, I gained a few pounds after taking it for 2 months. But because delayed stomach emptying makes me feel full when I've eaten relatively small amounts of food, it seems to make it much easier to eat at a low calorie level I have found impossible in the past.
In the past, when I've dieted, I've always cut my carbs way down. But what I found during the first few days on this diet, when I was restricting carbs more stringently, was this: if I don't eat enough carbs to go over the threshold that stimulates GLP-1-mediated first phase insulin response, my blood sugars throughout the day will be higher than if I do eat those carbs. So I do a lot better as far as blood sugars go, while taking Januvia, when eating 30 grams per meal than I do eating 10.
I also find that, as I've learned in the past, my fasting bgs are a bit better if I eat a slightly carby snack before bed--say a pretzel log. But since I've also learned that I diet best if I only eat at meals, I haven't been eating in the evening, so my fasting bg is in the 90s again, rather than the 80s. However, during the day, my blood sugar two hours after eating and until I eat again remains in the low 80s, sometimes even the 70s.
As a result, my total meter average has declined to 94 over the past 2 weeks, from 96 for the month, but my fasting bg for the week is up to 90 from 88 while after meals average is down 1 to 99 from 100. Since my meter average at the end of the period when I was taking insulin was 103, I'm very happy with all these figures (I didn't have a meter that distinguished before and after meals back then.)
After 2 weeks, I am back o my target weight, which suggests that some of the weight gain was water weight, but I'm doing so well with the diet, I'm going to put in another week and see how much lower I can get since it's not all that difficult. However, before I do that, I'm going to eat normally today and possibly tomorrow.
That's because eating at such a low calorie level is likely to slow my metabolism, a common problem with diets, and I don't want to start gaining weight when I go back to eating the 1600 calorie a day diet on which I've maintained so nicely through the last 4 years.
My final comment is that going from 12 grams of carbs (on a LC regimen) to a 30 gram carb intake makes the difference between a diet that feels very stringent and one where I literally, as they say in the crappy infomercials, "lose weight eating all my favorite foods." I've been eating toast for breakfast and 100 g of diet ice cream for dessert, with other occasional "treats" including 4 ounces of a bakery eclair. All weighed and counted--and with no blood sugar over 105 at 1 hour except once, when I saw 119 mg/dl.
That 119 mg/dl occurred several hours after eating, when I got very dizzy from too low a blood pressure and ended up with a counterregulatory response that pushed up both blood pressure, pulse, and blood sugar. Not after eating carbs! It looks like my weird surge of high blood pressure is fading some and starting to see the medication pushing me too low which is what has happened in the past.
Meanwhile, the seedlings are growing by the window sill, the 15 inches of snow on my back yard are enjoying one last wintry blast before next week's temperatures rise into he 40s and 50s, and pretty soon I'll be out in my garden, using up a lot more physical energy and reveling in the wonder that is the New England spring!
March 9, 2007
Research Gives More Insight into "What is a Normal Blood Sugar"
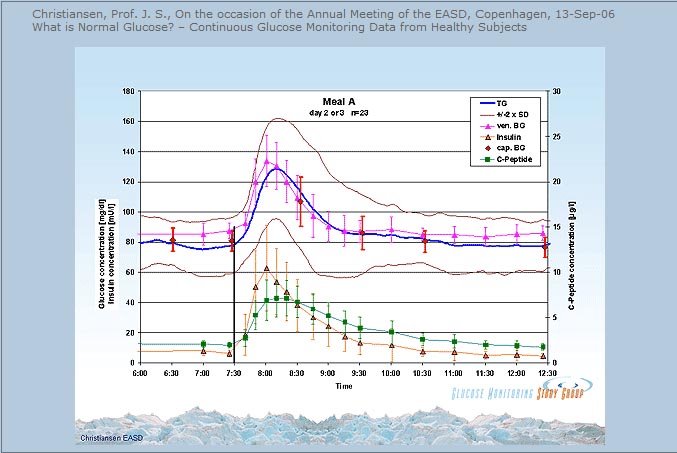
Here's an illuminating research study that was presented at a major European conference in September, 2006. It reports on the daily pattern of blood sugars of a group of normal subjects as revealed by continuous blood sugar monitoring. It gives a very solid answer to the question, "What is a normal blood sugar?"
What is Normal Glucose? – Continuous Glucose Monitoring Data from Healthy Subjects. Professor J.S. Christiansen, presented at the Annual Meeting of the EASD.
Above is a very revealing graph screen-captured from the dynamic display of this presentation. Click on the image to enlarge it so you can read it better.
It shows analysis of data from a study of normal people's blood sugars after a high carbohydrate breakfast eaten at 7:30 AM. The blue line is the average for the group. The brown lines are the readings for the people with the highest and lowest individual values which very possibly are those with the highest (5.4%) and lowest (4.3%) A1Cs.
The main findings here, for those of you who don't have the high speed internet connection needed to listen to this presentation, is that in normal people fasting blood glucose throughout the night stays flat in the low 80 mg/dl (4.4 mmol/L) range. After a high carb meal, blood sugar rises to about 125 mg/dl for a brief period, with the peak blood sugar being measured at 45 minutes after eating. The chart at the top of this page is taken from this presentation. Notice that in all but the people with the highest A1cs, blood sugar is under 100 mg/dl (5.5 mmol/L) at 1 hour and 15 minutes after eating and it returns to 85 mg/dl (4.7 mmol/L) by 1 hour and 45 minutes after eating.
Note also, how much lower even the highest of these normal readings are than the ADA's diagnostic cutoff for "impaired glucose tolerance" which is 140 mg/dl two hours after eating!
A few people in the study went as high as 160 mg/dl (8.9 mmol/L) after the high carb meal, which may be because they are not entirely normal. The study most likely recruited normal subjects based on their A1cs and the highest values in the group went up to 5.4% which is compatible with very early deterioration in first phase insulin secretion.
This study also documents that eating a high carb meal for breakfast results in an unacceptably high blood sugar swing much higher than any other blood sugar rise seen throughout the day, even for normal people, a point that the professor stresses in his presentation. So throw out the Corn Flakes!
March 7, 2007
More Evidence that Common Over-The-Counter Pain Pills are Toxic to the Kidney
This week's Diabetes in Control newsletter reports on a new study that finds that daily use of common painkillers including Tylenol (acetaminophen), Ibuprofen (Motrin) and even aspirin raise the incidence of high blood pressure very significantly.
Here is what "Diabetes in Control" wrote in their summary of this study, published in February in Archives of Internal Medicine (and hence, alas, not available in full text to us proles without subscriptions.)
"John P. Forman, MSc, MD, of Brigham and Women's Hospital and Harvard Medical School, Boston, and colleagues followed a total of 16,031 male health professionals (average age 64.6 years) who did not have a history of high blood pressure. The men were asked in 2000 and again in 2002 about whether and how often they used three types of pain relievers: acetaminophen, NSAIDs and aspirin. They were also asked to report if their physician had diagnosed them with hypertension.
"Over four years of follow-up, 1,968 men developed hypertension. Compared with men who did not take analgesics, those who took acetaminophen six or seven days a week had a 34% higher risk of hypertension. Those who took NSAIDs six or seven days a week had a 38% higher risk and those who took aspirin six or seven days a week had a 26% higher risk."
High blood pressure is often the very first sign of kidney dysfunction, though doctors continue to treat high blood pressure as "idiopathic" (doctor speak for "we have no clue what causes it.")
Coming on top of an earlier study which found that there is clear-cut relationship between your lifetime dose of acetaminophen and NSAID painkillers like ibuprofen and your likelihood of suffering total kidney failure (End Stage Renal Disease or ESRD), this should be a wake-up call to anyone who still pops a pain pill any time they have the slightest bit of discomfort.
How many pain pills are damaging? According to this study published in the New England Journal of Medicine, a lot less than you might think:
"When persons who took an average of 0 to 104 pills [of acetaminophen] per year were used for reference, the odds ratio of ESRD was 1.4 (95 percent confidence interval, 0.8 to 2.4) for those who took 105 to 365 pills per year and 2.1 (95 percent confidence interval, 1.1 to 3.7) for those who took 366 or more pills per year, after adjustment for race, sex, age, and intake of other analgesic drugs."
What this means in English is that taking one Tylenol pill every three days throughout the year is enough to give you a significantly increased risk for ending up on dialysis. And remember, this finding applied to a normal population, not people with diabetes who already have an increased risk for kidney failure.
The study also found "When persons who had taken fewer than 1000 pills containing acetaminophen in their lifetime were used for reference, the odds ratio [for developing end stage renal disease] was 2.0 (95 percent confidence interval, 1.3 to 3.2) for those who had taken 1000 to 4999 pills and 2.4 (95 percent confidence interval, 1.2 to 4.8) for those who had taken 5000 or more pills."
This means that you are twice as likely to end up on dialysis if you take between 1000 and 4999 Tylenol or acetaminophen pills during your entire lifetime!. That's slightly over ten bottles of pills. Over your lifetime!
The study also found "A cumulative dose of 5000 or more pills containing NSAIDs was also associated with an increased odds of ESRD (odds ratio, 8.8)." This refers to drugs like ibuprofen and naproxen (sold as Motrin and Anaprox.)
The NEJM article did not find a relationship between lifetime dose of aspirin and kidney failure, but it's worth noting that the new study did find that taking aspirin daily did go along with the development of high blood pressure.
Looks like it's time to stop popping "vitamin I" every time you feel a little sore.
Save the painkillers for when you are really in pain and then if you must take a pill, take the smallest pill that will get the job done. I find that one 325 mg regular strength Tylenol is all I need when I have serious nerve pain from my ruptured disc. Taking more does not increase the relief. But I also find I have to hunt for the regular strength version of the drug, since the pharmacies clearly believe "more is better" and most of the bottles on the pain reliever shelf are "extra strength" versions that contain at least twice as much drug per pill.
If you require long term pain treatment for a chronic condition like arthritis, raise the issue with your doctor of whether there is some other class of drugs available that might be less dangerous for your kidneys. I did this when I was having a rough time with nerve compression in my frozen shoulder and ended up using Tramadol to help me sleep. Tramadol is usually considered a heavy duty drug, but it worked, and when the pain abated after six weeks I had no trouble stopping it. I did take Tylenol when the pain got really bad during the day, since it is very effective for nerve pain, but I tried to limit myself to no more than 2 pills a day, and less if I could, because I knew it was going to be a while until the problem resolved and I really like having functional kidneys.
Here is what "Diabetes in Control" wrote in their summary of this study, published in February in Archives of Internal Medicine (and hence, alas, not available in full text to us proles without subscriptions.)
"John P. Forman, MSc, MD, of Brigham and Women's Hospital and Harvard Medical School, Boston, and colleagues followed a total of 16,031 male health professionals (average age 64.6 years) who did not have a history of high blood pressure. The men were asked in 2000 and again in 2002 about whether and how often they used three types of pain relievers: acetaminophen, NSAIDs and aspirin. They were also asked to report if their physician had diagnosed them with hypertension.
"Over four years of follow-up, 1,968 men developed hypertension. Compared with men who did not take analgesics, those who took acetaminophen six or seven days a week had a 34% higher risk of hypertension. Those who took NSAIDs six or seven days a week had a 38% higher risk and those who took aspirin six or seven days a week had a 26% higher risk."
High blood pressure is often the very first sign of kidney dysfunction, though doctors continue to treat high blood pressure as "idiopathic" (doctor speak for "we have no clue what causes it.")
Coming on top of an earlier study which found that there is clear-cut relationship between your lifetime dose of acetaminophen and NSAID painkillers like ibuprofen and your likelihood of suffering total kidney failure (End Stage Renal Disease or ESRD), this should be a wake-up call to anyone who still pops a pain pill any time they have the slightest bit of discomfort.
How many pain pills are damaging? According to this study published in the New England Journal of Medicine, a lot less than you might think:
"When persons who took an average of 0 to 104 pills [of acetaminophen] per year were used for reference, the odds ratio of ESRD was 1.4 (95 percent confidence interval, 0.8 to 2.4) for those who took 105 to 365 pills per year and 2.1 (95 percent confidence interval, 1.1 to 3.7) for those who took 366 or more pills per year, after adjustment for race, sex, age, and intake of other analgesic drugs."
What this means in English is that taking one Tylenol pill every three days throughout the year is enough to give you a significantly increased risk for ending up on dialysis. And remember, this finding applied to a normal population, not people with diabetes who already have an increased risk for kidney failure.
The study also found "When persons who had taken fewer than 1000 pills containing acetaminophen in their lifetime were used for reference, the odds ratio [for developing end stage renal disease] was 2.0 (95 percent confidence interval, 1.3 to 3.2) for those who had taken 1000 to 4999 pills and 2.4 (95 percent confidence interval, 1.2 to 4.8) for those who had taken 5000 or more pills."
This means that you are twice as likely to end up on dialysis if you take between 1000 and 4999 Tylenol or acetaminophen pills during your entire lifetime!. That's slightly over ten bottles of pills. Over your lifetime!
The study also found "A cumulative dose of 5000 or more pills containing NSAIDs was also associated with an increased odds of ESRD (odds ratio, 8.8)." This refers to drugs like ibuprofen and naproxen (sold as Motrin and Anaprox.)
The NEJM article did not find a relationship between lifetime dose of aspirin and kidney failure, but it's worth noting that the new study did find that taking aspirin daily did go along with the development of high blood pressure.
Looks like it's time to stop popping "vitamin I" every time you feel a little sore.
Save the painkillers for when you are really in pain and then if you must take a pill, take the smallest pill that will get the job done. I find that one 325 mg regular strength Tylenol is all I need when I have serious nerve pain from my ruptured disc. Taking more does not increase the relief. But I also find I have to hunt for the regular strength version of the drug, since the pharmacies clearly believe "more is better" and most of the bottles on the pain reliever shelf are "extra strength" versions that contain at least twice as much drug per pill.
If you require long term pain treatment for a chronic condition like arthritis, raise the issue with your doctor of whether there is some other class of drugs available that might be less dangerous for your kidneys. I did this when I was having a rough time with nerve compression in my frozen shoulder and ended up using Tramadol to help me sleep. Tramadol is usually considered a heavy duty drug, but it worked, and when the pain abated after six weeks I had no trouble stopping it. I did take Tylenol when the pain got really bad during the day, since it is very effective for nerve pain, but I tried to limit myself to no more than 2 pills a day, and less if I could, because I knew it was going to be a while until the problem resolved and I really like having functional kidneys.
Subscribe to:
Comments (Atom)

